accuracy of acetabular labrum tear tests trial|acetabular labral treatment : department Store Labral tears have been well documented in people with hip dysplasia [7, 39, 50, 73, 76]. In a study of patients with mild-to-moderate hip dysplasia and hip pain, McCarthy and Lee found that 72% of the 170 hips studied had labral tears, and 93% of these tears were in the anterior region of the labrum [76]. The preferred orientation for pouches is resting on their edge best accomplished using the Midmark pouch rack accessory. If using the standard tray, pouches should be placed paper side down. All items must be .
{plog:ftitle_list}
According to the Association of periOperative Registered Nurses’ (AORN) guidelines1, peel pouches should be placed on an edge and spaced to permit sterilant contact and drying when loading the sterilizer.
A more recent study in those with acetabular labral tear has shown that conservative management over the course of 1 year with corticosteroid injection, activity modification, and physical therapy led to improved functional outcomes, and 71% of patients . A more recent study in those with acetabular labral tear has shown that conservative management over the course of 1 year with corticosteroid injection, activity modification, and physical therapy led to improved functional outcomes, and 71% of patients were satisfied with nonsurgical treatment. The purpose of this study was to determine (1) the diagnostic accuracy of MRI and MRA for the detection of ALT, (2) whether 1.5 T or 3.0 T is all acceptable, by conducting a meta-analysis of the literature regarding the diagnostic performance of MRI/MRA.Labral tears have been well documented in people with hip dysplasia [7, 39, 50, 73, 76]. In a study of patients with mild-to-moderate hip dysplasia and hip pain, McCarthy and Lee found that 72% of the 170 hips studied had labral tears, and 93% of these tears were in the anterior region of the labrum [76].
For MRI (eight studies), the pooled sensitivity for detecting acetabular labral tears was 66% (95% CI 59 to 73) and pooled specificity was 79% (95% CI 67 to 91). For MRA (15 studies), the pooled sensitivity was 87% (95% CI 84 to 90) and pooled specificity was 64% (95% CI 54 to 74).
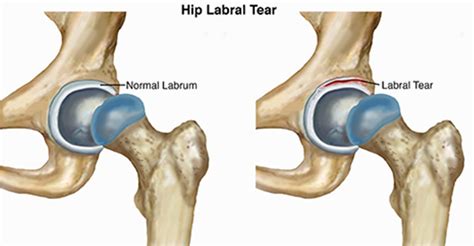
The objective of the study was to determine diagnostic accuracy and validity of the patient history, physical examination and imaging for the diagnosis of acetabular labral tears in patients presenting with hip pain. Acetabular labral tears may occur because of abnormal bony morphology (femoroacetabular impingement or secondary proximal femoral deformity), dysplasia, capsular laxity, trauma, or degeneration.
We included all diagnostic accuracy studies that directly compared within-study, the accuracy of MRI or MRA (the index tests), to either arthroscopic or open surgical findings (the reference test) relating to acetabular labral tears.The meta-analysis demonstrated that flexion-adduction-internal rotation (pooled SN ranging from 0.94 (95% CI 0.90 to 0.97) to 0.99 (95% CI 0.98 to 1.00); DOR 5.71 (95% CI 0.84 to 38.86) to 7.82 (95% CI 1.06 to 57.84)) and flexion-internal rotation (pooled SN 0.96 (95% CI 0.81 to 0.99); DOR 8.36 (95% CI 0.41 to 171.3) tests possess only .
mri for acetabular labral tears
With physiotherapy, the mean iHOT12 score of the 35 patients with acetabular labral tears showed significant improvement from 44.0 to 73.6 ( P <0.001) in 4.7 months. Of these 35 patients, eight patients (22.9%) underwent surgical .Park SY et al. compared the diagnostic accuracy of three-dimensional intermediate-weighted fast spin-echo sequence and two-dimensional fast spin-echo sequences for the diagnosis of acetabular labral tears, and they found that Se and Sp were 0.74 and 0.89 for two-dimensional fast spin-echo sequences, and 0.78 and 0.92 for three-dimensional . A more recent study in those with acetabular labral tear has shown that conservative management over the course of 1 year with corticosteroid injection, activity modification, and physical therapy led to improved functional outcomes, and 71% of patients were satisfied with nonsurgical treatment.
The purpose of this study was to determine (1) the diagnostic accuracy of MRI and MRA for the detection of ALT, (2) whether 1.5 T or 3.0 T is all acceptable, by conducting a meta-analysis of the literature regarding the diagnostic performance of MRI/MRA.
Labral tears have been well documented in people with hip dysplasia [7, 39, 50, 73, 76]. In a study of patients with mild-to-moderate hip dysplasia and hip pain, McCarthy and Lee found that 72% of the 170 hips studied had labral tears, and 93% of these tears were in the anterior region of the labrum [76].

For MRI (eight studies), the pooled sensitivity for detecting acetabular labral tears was 66% (95% CI 59 to 73) and pooled specificity was 79% (95% CI 67 to 91). For MRA (15 studies), the pooled sensitivity was 87% (95% CI 84 to 90) and pooled specificity was 64% (95% CI 54 to 74).The objective of the study was to determine diagnostic accuracy and validity of the patient history, physical examination and imaging for the diagnosis of acetabular labral tears in patients presenting with hip pain. Acetabular labral tears may occur because of abnormal bony morphology (femoroacetabular impingement or secondary proximal femoral deformity), dysplasia, capsular laxity, trauma, or degeneration. We included all diagnostic accuracy studies that directly compared within-study, the accuracy of MRI or MRA (the index tests), to either arthroscopic or open surgical findings (the reference test) relating to acetabular labral tears.
The meta-analysis demonstrated that flexion-adduction-internal rotation (pooled SN ranging from 0.94 (95% CI 0.90 to 0.97) to 0.99 (95% CI 0.98 to 1.00); DOR 5.71 (95% CI 0.84 to 38.86) to 7.82 (95% CI 1.06 to 57.84)) and flexion-internal rotation (pooled SN 0.96 (95% CI 0.81 to 0.99); DOR 8.36 (95% CI 0.41 to 171.3) tests possess only . With physiotherapy, the mean iHOT12 score of the 35 patients with acetabular labral tears showed significant improvement from 44.0 to 73.6 ( P <0.001) in 4.7 months. Of these 35 patients, eight patients (22.9%) underwent surgical .
how to read a refractive index on a refractometer
how to read a refractometer beer
$2,268.99
accuracy of acetabular labrum tear tests trial|acetabular labral treatment